Malaria – tiny bite, major effect

Along with tuberculosis and AIDS, malaria is one of the “big three”, the three infectious diseases that are globally responsible for most deaths. According to World Health Organization estimates, some 282 million cases of malaria and more than 600,000 deaths were reported in 2026 alone. More than 90% of infections and deaths occur in Africa. Children are at an especially high risk as their immune system is not yet familiar with the disease.
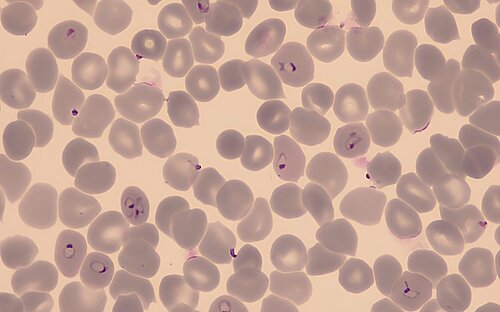
The risk of infection is highest at night as this is the prime time for the Anopheles mosquito to bite and, simultaneously, transmit Plasmodium, the malaria pathogen. An infected female mosquito namely not only sucks blood - it also injects sporozoites, which represent one of the infective forms of the single-celled parasite.
One parasite, many life forms
In humans and the Anopheles mosquito, Plasmodium goes through different developmental stages. A mosquito bite transmits the sporozoites into the human circulation where the parasite initially develops and proliferates inside liver cells and, thereafter, inside red blood cells, also known as erythrocytes, which supply vital oxygen to our cells. Inside erythrocytes, Plasmodium matures to its sexually reproductive gametocyte stage. If, during a blood meal, the Anopheles mosquito feeds on an infected person's blood, red blood cells containing gametocytes end up in the midgut of the mosquito, the site of sexual reproduction. The life cycle completes a full circle when the pathogen migrates to the salivary glands of the mosquito, ready to infect its next victim. This way, the mosquito has effectively become a "vector", transmitting the pathogen - and with it the disease - from person to person.
Special climatic conditions are required for the proliferation of the Anopheles mosquito and for Plasmodium to go through the different stages of its life cycle. Ideal conditions exist in tropical and subtropical regions. Over 40 % of world’s population lives in these malaria endemic areas.
During the parasite life cycle, infected erythrocytes burst on a regular basis, often simultaneously, allowing the released parasites to infect new red blood cells. Along with the single-celled parasites, toxic metabolites end up in the bloodstream, leading to periodic fevers, nausea, and headaches – the typical symptoms of malaria that can be traced back to the immune response. This inflammatory response is significantly abated in patients who are, on one set of their chromosomes, carriers of the gene for a disease called sickle cell anemia. In these individuals, part of their oxygen-carrying proteins are structurally defective, and some erythrocytes assume a sickled shape, hence the name of the disease. As the underlying mutation protects carriers from malaria, sickle cell anemia is highly prevalent in areas where malaria is endemic.
Different Plasmodium species cause malaria in humans
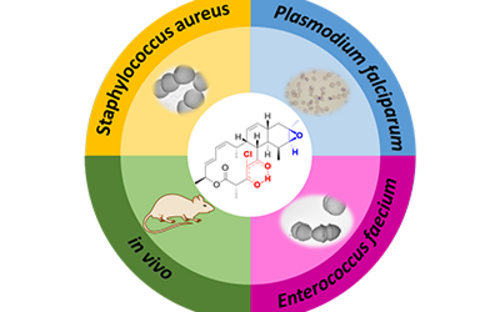
There are four known species of Plasmodium that can cause malaria in humans: Plasmodium falciparum, Plasmodium vivax, Plasmodium malariae, and Plasmodium ovale. One other species, Plasmodium knowlesi, primarily infects monkeys but can also affect humans. Plasmodium falciparum, the pathogen that causes Malaria tropica, is considered especially dangerous as it leads to a range of complications. Left untreated, this form is fatal in up to 20 % of cases. However, it can be effectively treated with combination therapy using different artemisinin-containing drugs. As resistance to these common therapeutics is increasingly being observed, there is an urgent need for research into new active substances. At the Helmholtz Institute for Pharmaceutical Research Saarland (HIPS), researchers have discovered that substances from the natural product class of chlorotoniles are not only effective against various hospital germs, but also against Plasmodium falciparum. Together with partners from the University Hospital Tübingen, they are now working on optimizing the active substances for the treatment of malaria.
Finally, an approved vaccine…
The best prevention is to avoid getting bitten by the mosquito using protection, such as mosquito nets and insecticide sprays. However, in recent years, another alternative for protecting children has finally become available: in October 2021, the WHO recommended the use of the RTS,S vaccine in areas where malaria is endemic. With a total of four vaccine doses, three of which are administered in the first year of life and one booster dose at around the age of 2, up to 75% of malaria cases in children can be prevented. Since 2023, another vaccine with comparable efficacy has been available: R21. Further vaccine candidates are in development and clinical trials.
Climate change may cause malaria endemic areas to shift in the future. Extreme weather events with flooding can create new breeding grounds for the mosquitoes that transmit the disease. However, if we succeed in combining new drugs with widespread access to vaccines, we will have effective tools at our disposal to combat this notorious infectious disease and save many lives.
Status: March 2026
(bma, cwe)
Further Information
FAQ by the WHO on malaria vaccines
Involved research groups
-
Microbial Natural Products
 Prof Dr Rolf Müller
Prof Dr Rolf Müller -
Drug Design and Optimization
 Prof Dr Anna K. H. Hirsch
Prof Dr Anna K. H. Hirsch